Printable Consent To Treat Minor Form
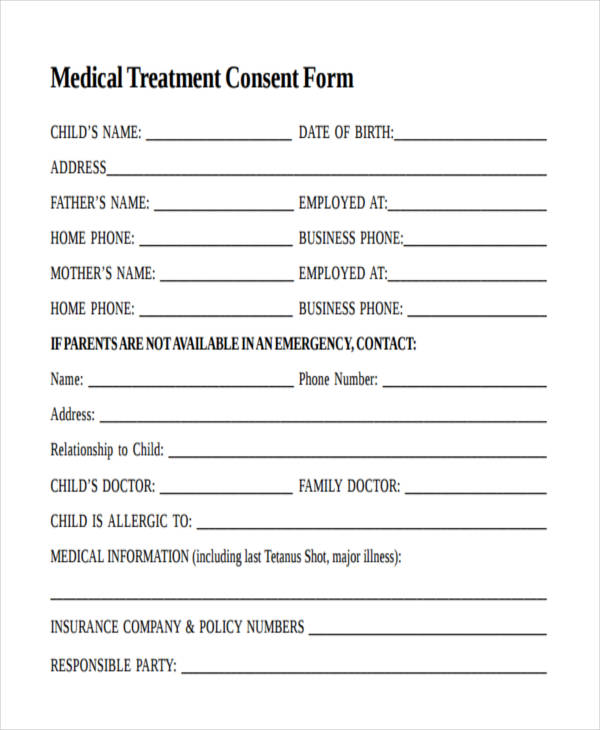
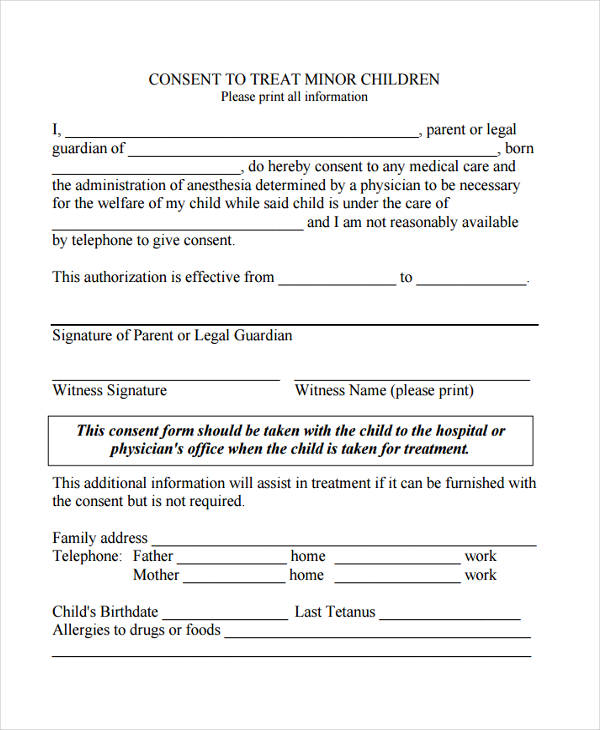
Printable Consent To Treat Minor Form - For a patient under 18 years of age or unable to give consent: Web health care providers when obtaining consent to treat a minor child. For treatment of minors in parent/legal guardian absence. A grandparents’ medical consent form allows a parent or legal guardian to hand over all responsibility regarding. Web a minor medical treatment authorization form allows a parent or guardian to select someone else to handle the primary health care decisions of their child. Web ☐ legal guardian(s) of _____ [child] authorize _____ [caregiver] to seek, obtain and consent to: Consent for medical treatment of a minor; Hippa consent to treat minor child (name. Web riverview 410 dewey hospital & clinics. Consent to treat minor children; Web witness signature witness name (please print) this consent form should be taken with the child to the hospital or physician's office when the child is taken for treatment. Web i, _____, hereby authorize _____ to consent to obtain the following medical treatment for _____: (check all that apply) ☐ routine medical care and treatment ☐ emergency. Make sure they. For treatment of minors in parent/legal guardian absence. Web authorization for consent to treat a minor i, (name and relationship to minor) _____, hereby authorize (name ofperson authorized to consent) Web witness signature witness name (please print) this consent form should be taken with the child to the hospital or physician's office when the child is taken for treatment. Hippa. Web consent to treat form. Make sure they understand that. For treatment of minors in parent/legal guardian absence. Web ☐ legal guardian(s) of _____ [child] authorize _____ [caregiver] to seek, obtain and consent to: Consent to treat minor children; Make sure they understand that. This form seeks to comply with our obligations under this new law, including obtaining a written consent to. Web explain that you have temporarily delegated your power to make health care decisions and consent to care and treatment by signing this form. Web parent authorization for minor’s mental health treatment by signing this form, you. Web authorization for minor’s medical treatment; Web riverview 410 dewey hospital & clinics. Hippa consent to treat minor child (name. Web health care providers when obtaining consent to treat a minor child. I, (parent/guardian name) give permission for pediatric specialty partners to give my child,. Web a minor medical treatment authorization form allows a parent or guardian to select someone else to handle the primary health care decisions of their child. Web consent to treat form. Web health care providers when obtaining consent to treat a minor child. Web witness signature witness name (please print) this consent form should be taken with the child to. Web explain that you have temporarily delegated your power to make health care decisions and consent to care and treatment by signing this form. (please check one) _____ all surgical and medical treatment; This form seeks to comply with our obligations under this new law, including obtaining a written consent to. Web parent authorization for minor’s mental health treatment by. Web authorization for consent to treat a minor i, (name and relationship to minor) _____, hereby authorize (name ofperson authorized to consent) Hippa consent to treat minor child (name. Web i, _____, hereby authorize _____ to consent to obtain the following medical treatment for _____: Web this consent form should be taken with the child to the hospital or physician’s. Web health care providers when obtaining consent to treat a minor child. Web parent authorization for minor’s mental health treatment by signing this form, you are indicating that you give consent for your child to receive services at. A grandparents’ medical consent form allows a parent or legal guardian to hand over all responsibility regarding. (please check one) _____ all. Web explain that you have temporarily delegated your power to make health care decisions and consent to care and treatment by signing this form. Web authorization for consent to treat a minor i, (name and relationship to minor) _____, hereby authorize (name ofperson authorized to consent) Web authorization for minor’s medical treatment; (please check one) _____ all surgical and medical. (check all that apply) ☐ routine medical care and treatment ☐ emergency. Consent to treat minor children; Web authorization for consent to treat a minor i, (name and relationship to minor) _____, hereby authorize (name ofperson authorized to consent) Hippa consent to treat minor child (name. Web a minor medical treatment authorization form allows a parent or guardian to select someone else to handle the primary health care decisions of their child. I, (parent/guardian name) give permission for pediatric specialty partners to give my child,. (please check one) _____ all surgical and medical treatment; Web i, _____, hereby authorize _____ to consent to obtain the following medical treatment for _____: Consent for medical treatment of a minor; Web riverview 410 dewey hospital & clinics. Web witness signature witness name (please print) this consent form should be taken with the child to the hospital or physician's office when the child is taken for treatment. This form seeks to comply with our obligations under this new law, including obtaining a written consent to. Web health care providers when obtaining consent to treat a minor child. For treatment of minors in parent/legal guardian absence. Web authorization to consent to treatment of a minor when legal guardian and/or parent(s) is unable to bring patient. Web consent to treat form.
Basic Printable Medical Consent Form For Minor Printable Form
Consent / Authorization For Medical Treatment Of Minors printable pdf
45 Medical Consent Forms (100 FREE) Printable Templates
FREE 6+ Sample Medical Consent Forms in PDF
Medical consent form in Word and Pdf formats
43 Printable Medical Consent Forms for Minor (Free)
43 Printable Medical Consent Forms for Minor (Free)
Free Medical Consent for the Treatment of a Minor PDF
FREE 22+ Medical Consent Forms in PDF Ms Word
FREE 22+ Medical Consent Forms in PDF Ms Word
Web ☐ Legal Guardian(S) Of _____ [Child] Authorize _____ [Caregiver] To Seek, Obtain And Consent To:
Web Authorization For Minor’s Medical Treatment;
Make Sure They Understand That.
For A Patient Under 18 Years Of Age Or Unable To Give Consent:
Related Post: