Nursing Charting Examples
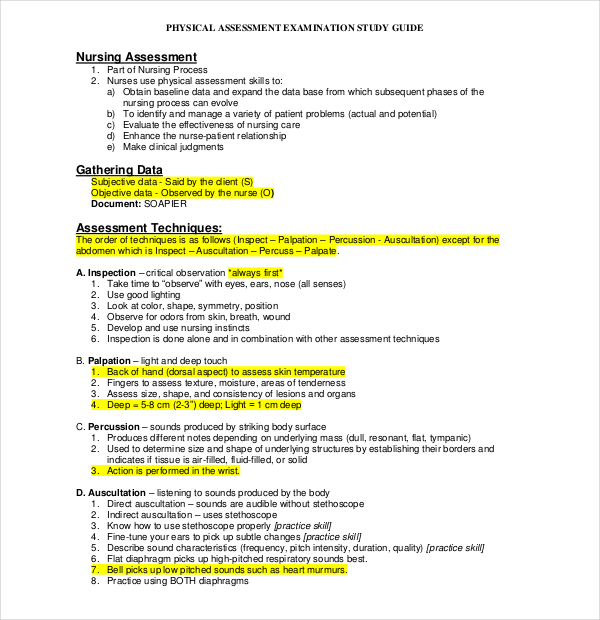
Nursing Charting Examples - No known allergies/no known drug allergies. Patient’s abdomen is soft, nondistended, and bowel sounds are present in all four quadrants. Patient denies cough, chest pain, or shortness of breath. Your assessment of the patient: See different examples of nursing notes and discover tips to improve your documentation skills. Nursing documentation is an essential aspect of patient care and plays a pivotal role in enhancing communication between healthcare professionals, recording medical history accurately, and providing legal protection for registered nurses (rns). Be precise with your notation. Web some commonly accepted abbreviations and acronyms for nurse charting purposes include: Sample documentation of expected findings. Head of the bed elevated to 45 degrees. Soapie stands for subjective, objective, assessment, plan, intervention, and evaluation. What your assessment told you. Avoid repetitive copying and pasting. To use email share, please make sure your browser pop up blocker is turned off. Web for example, a tin of baked beans costs $5.80, compared with the current online price of $2.80 at coles and woolworths. 10 helpful nurse charting tips for nurses. Be precise with your notation. Your assessment of the patient: This might include a description of a nursing visit, a specific care event, or a summary of care. What your assessment told you. Web is nurse charting the bane of your existence? Patient’s abdomen is soft, nondistended, and bowel sounds are present in all four quadrants. Web give various examples for different charting scenarios. Web for example, a tin of baked beans costs $5.80, compared with the current online price of $2.80 at coles and woolworths. No known allergies/no known drug allergies. A nursing narrative note is a type of nursing documentation used to provide clear, detailed information about the patient. Web charting tips for nurses. This includes your interpretation of the findings and any diagnosis. Keep your notes simple and concise. It is a method of charting nurses use, along with other disciplines, to help focus on a specific patient problem,. Avoid these other common nurse documentation mistakes. Web give various examples for different charting scenarios. Genet liphart rhoads, ph.d, rn, cne. Keep paper handy to jot down notes. Many travelers are concerned with various charting systems that are utilized amongst different facilities. For example, the date/time the note was written, as well as your full name, credentials, and signature. It is geared to save time and decrease duplicate charting. Accurate documentation is crucial in the nursing profession, as it is the foundation for providing safe and effective care to patients. This includes your interpretation of the findings and any diagnosis. Web what. Patient denies cough, chest pain, or shortness of breath. Avoid repetitive copying and pasting. This includes your interpretation of the findings and any diagnosis. Web charting made easy: Patient’s abdomen is soft, nondistended, and bowel sounds are present in all four quadrants. Your assessment of the patient: Beef mince sells for $20 a kilo, double the going rate at a regular supermarket. Denies past or current respiratory illnesses or diseases. Genet liphart rhoads, ph.d, rn, cne. Web is nurse charting the bane of your existence? Avoid charting ahead of time. For example, the date/time the note was written, as well as your full name, credentials, and signature. This article will break down what soapie notes are and how to use them. It is geared to save time and decrease duplicate charting. This responsibility not only ensures legal compliance but also plays a significant role in. Avoid emotional or opinionated charting. Patient’s abdomen is soft, nondistended, and bowel sounds are present in all four quadrants. Web one of the most important parts of a nurse’s job is accurate, descriptive documentation. Web some examples of charting include documenting medications administered, vital signs, physical assessments, and interventions provided. Web what is nurse charting? Web what is nurse charting? A nursing narrative note is a type of nursing documentation used to provide clear, detailed information about the patient. These charts offer a structured approach to patient documentation that enhances clarity, communication, and continuity of care in healthcare settings. Soapie stands for subjective, objective, assessment, plan, intervention, and evaluation. Web charting tips for nurses. There are several different ways to write a nursing note, but this article will focus on one of the most popular and how it is written: Web in this article, i will share 5 nursing narrative note examples + how to write them and discuss the importance of accurate charting. Your assessment of the patient: Web for example, a tin of baked beans costs $5.80, compared with the current online price of $2.80 at coles and woolworths. To use email share, please make sure your browser pop up blocker is turned off. Make sure you follow hipaa policy. Avoid emotional or opinionated charting. For example, the date/time the note was written, as well as your full name, credentials, and signature. Denies past or current respiratory illnesses or diseases. This article will break the soapi note down so you can decide if it’s a format that will work for you. Keep paper handy to jot down notes.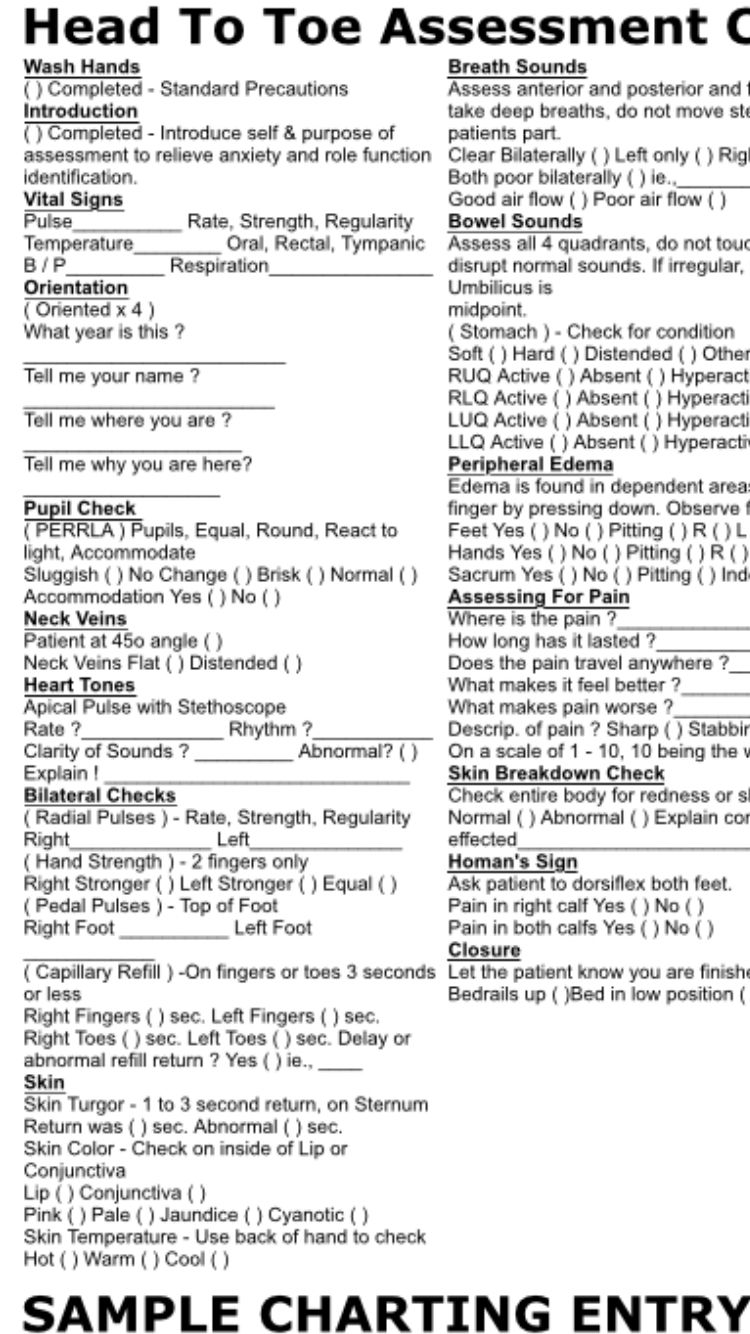
Nursing Student Head to Toe Assessment Cheat Sheet Sample Charting
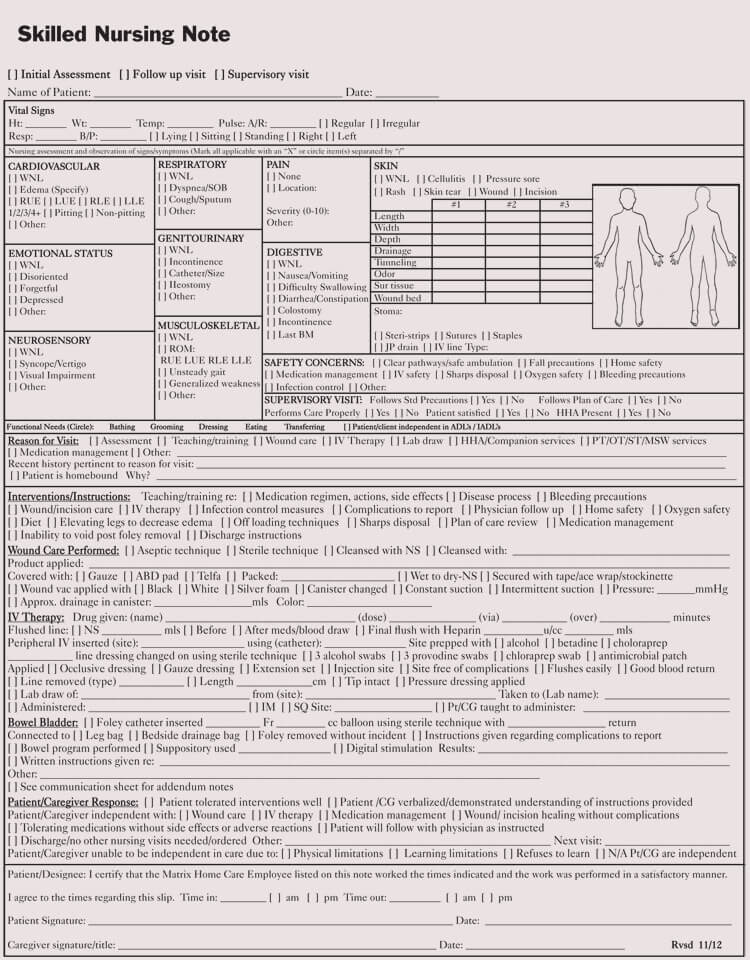
12+ Free Nursing Notes Templates (Guidelines to Take Nursing Notes)
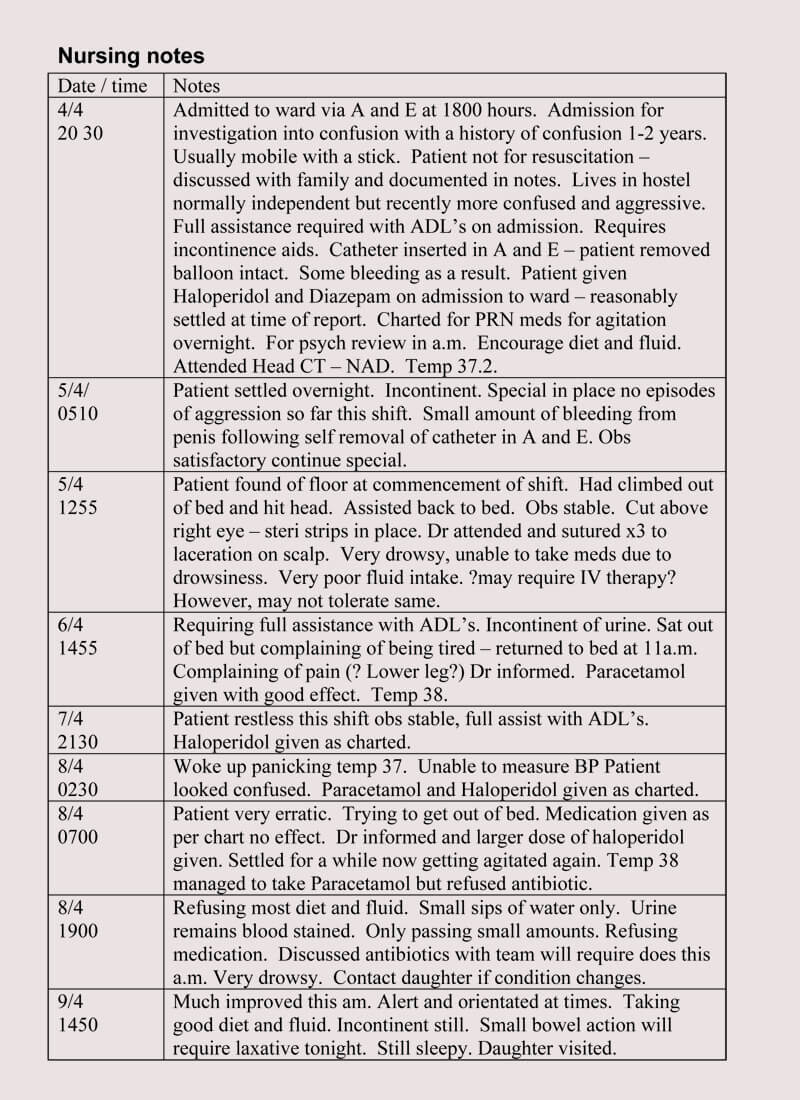
12+ Free Nursing Notes Templates (Guidelines to Take Nursing Notes)

the valley hospital timetable is shown in black and white

Nursing assessment Documentation Template Beautiful 197 Best Images
Nursing Charting Flow Sheet
12 HOW TO NURSING NOTES
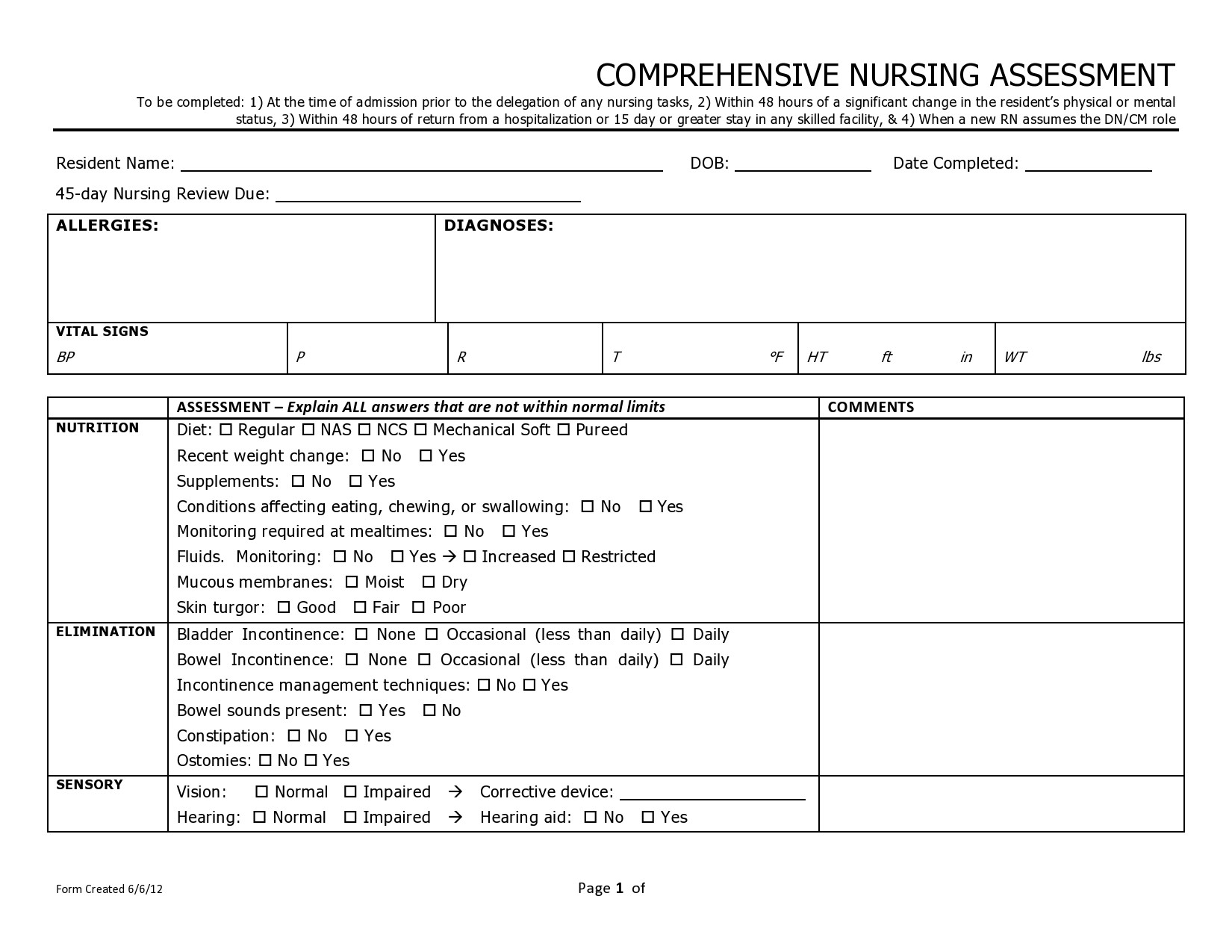
FREE 7+ Sample Nursing Assessment Forms in PDF MS Word
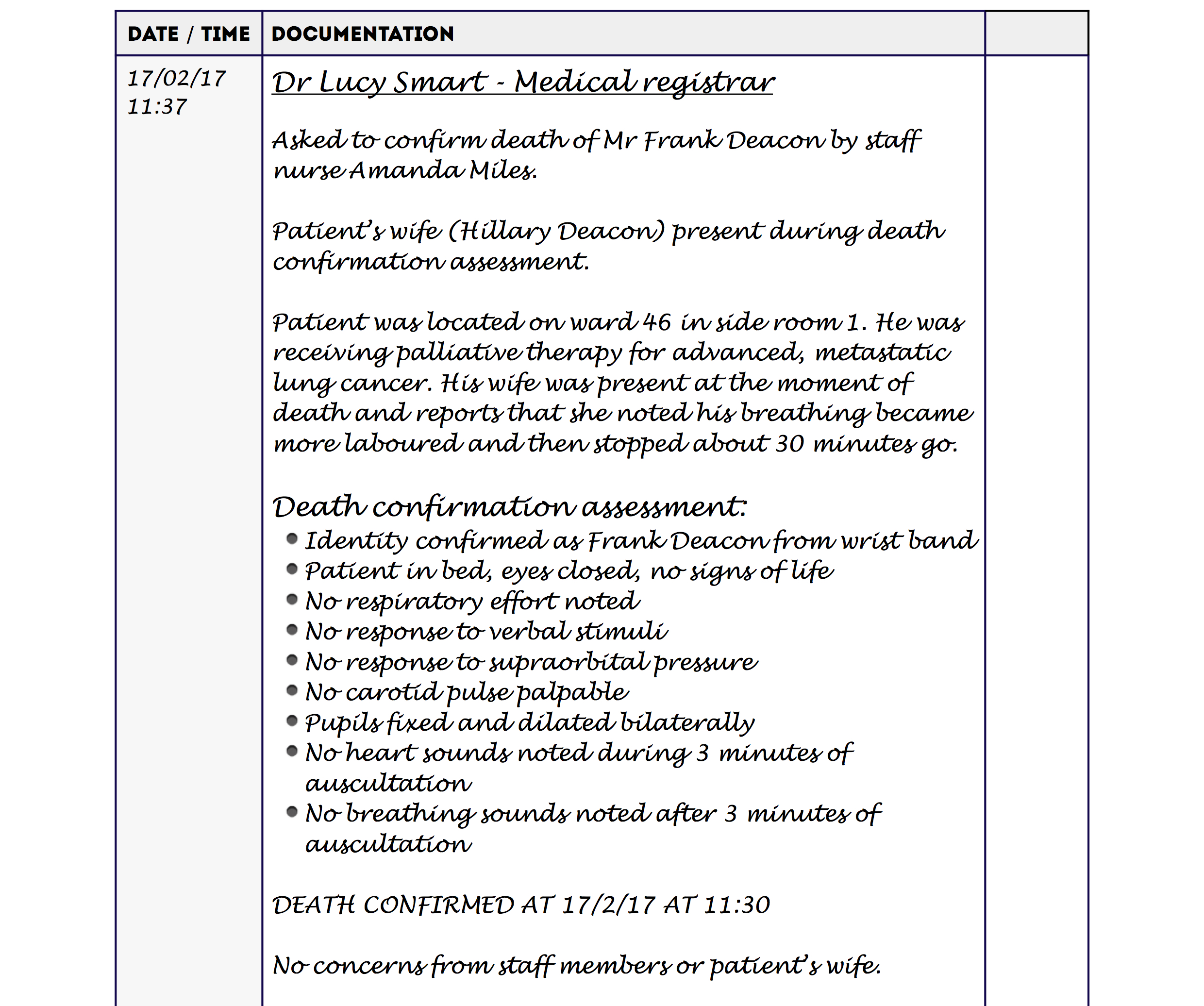
Nurses Notes Narrative Charting Sample Master of Template Document

Nursing Charting Template
Web Is Nurse Charting The Bane Of Your Existence?
It Is Geared To Save Time And Decrease Duplicate Charting.
10 Helpful Nurse Charting Tips For Nurses.
Ensure That Findings Are Properly Communicated And Acknowledged, Documenting These Actions In The Patient’s Health Information Record.
Related Post:
