Free Printable Flu Vaccine Consent Form
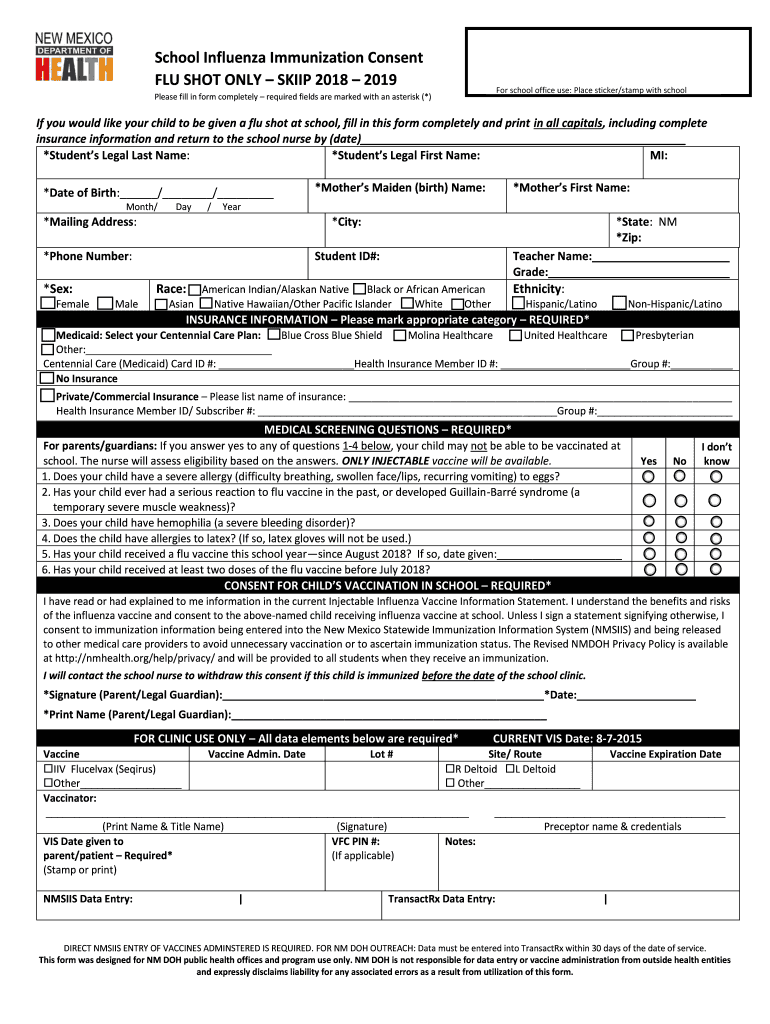
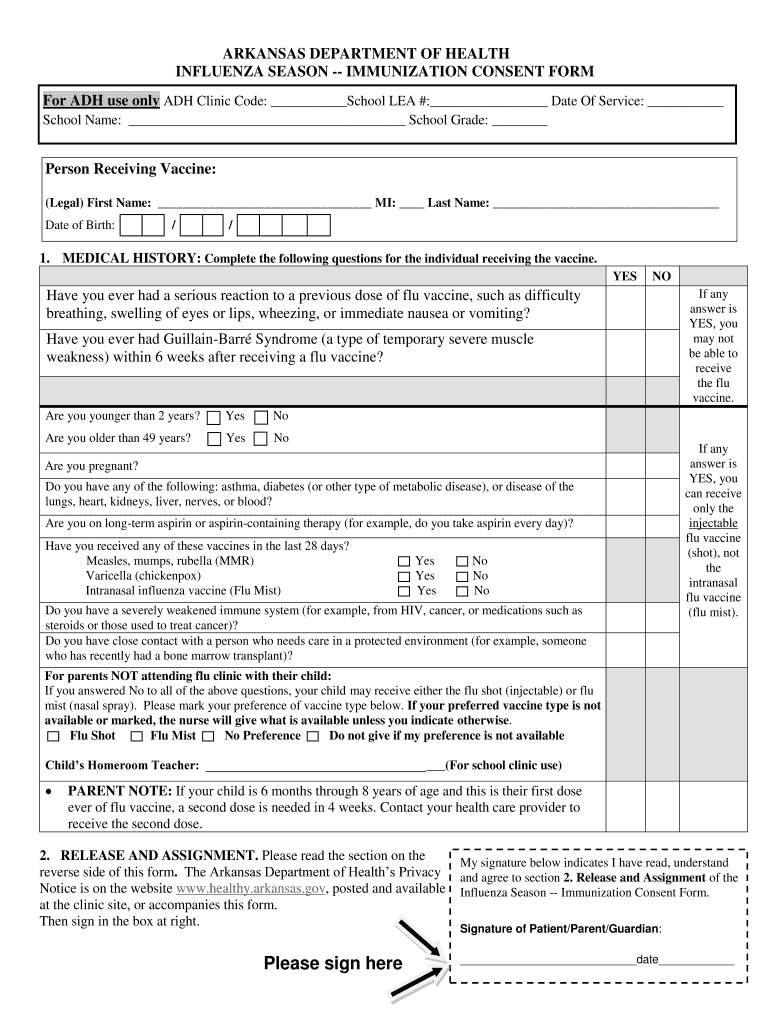
Free Printable Flu Vaccine Consent Form - Do any of the following apply? Norbert college (snc) health services department to give me named above the influenza vaccine. It should be signed by the patient, or, in the case of a minor, by a parent or legal guardian. Next year in 4 weeks other. _____/_____/____ (year, month, day) screening questions: Download free version (pdf format) download editable version for $3.99 (word format) download the entire collection for only $99. Web signature of recipient (parent or guardian) date. Web i consent to the administration of the influenza virus vaccine. Have you received the flu vaccine before? Dosage 0.5 ml 0.25 ml laiv. Web the information you provide to complete this form indicates you understand the benefits and risks of receiving the influenza vaccine, as indicated in the cdc's vaccine information statement (vis), and are requesting to be vaccinated. Dosage 0.5 ml 0.25 ml laiv. Influenza vaccine can prevent influenza (flu). When people get influenza they may have fever, chills, headache, dry cough,. Web i hereby consent to the administration of the flu vaccine for which i have signed below be given to me or the person named above for whom i am authorized pursuant to sections 431.058, 431.061 rsmo to make this request. First second if second, please indicate the date of the first dose: _____/______/____ (year, month, day) are you feeling. Influenza vaccine can prevent influenza (flu). First second if second, please indicate the date of the first dose: Do any of the following apply? I give my consent, voluntarily and of my own free will to the staff of st. _____/_____/____ (year, month, day) screening questions: Web i consent to the administration of the influenza virus vaccine. Even when the vaccine doesn’t exactly match these viruses, it may still provide some protection. Download free version (pdf format) download editable version for $3.99 (word format) download the entire collection for only $99. Web i hereby consent to the administration of the flu vaccine for which i have. Web influenza vaccine consent form. I have been given a copy of the vaccine information statement (vis). I have the legal authority to consent to have the minor patient named above vaccinated with the flu vaccine and am authorized to make health care decisions on behalf of the minor patient. This flu shot consent form is designed to by given. The vis publication date is 08/15/2019. Web baylor scott & white health. Web *for children 6 months of age to less than 9 years of age who have not been previously vaccinated with seasonal influenza vaccine, is this the first or second dose of seasonal influenza vaccine this year? First second if second, please indicate the date of the first. First second if second, please indicate the date of the first dose: The illness may last several days or longer. For children 6 months of age to less than 9 years of age who have not been previously vaccinated with seasonal influenza vaccine, is this the first or second dose of seasonal influenza vaccine this year? If second, please indicate. The illness may last several days or longer. Chat support availablecustomizable formsview pricing detailssearch forms by state Web i’ve had a chance to ask questions and they were answered to my satisfaction. Web ☐ i consent on behalf of the patient to receive the influenza vaccine today print name ____________________________________ relationship (if applicable) ______________________________ date _________________________________________ phone number. Web i. Administration date administration site left arm right arm nasal left thigh right thigh. Download free version (pdf format) download editable version for $3.99 (word format) download the entire collection for only $99. I reviewed this consent form and understand the potential risks and benefits of the influenza (flu) vaccine. _____/_____/____ (year, month, day) screening questions: The vis publication date is. Web i hereby consent to the administration of the flu vaccine for which i have signed below be given to me or the person named above for whom i am authorized pursuant to sections 431.058, 431.061 rsmo to make this request. Download free version (pdf format) download editable version for $3.99 (word format) download the entire collection for only $99.. Signature of person authorized to give consent. _____/_____/____ (year, month, day) screening questions: _____/______/____ (year, month, day) are you feeling ill today? Web i consent to the administration of the influenza virus vaccine. Chat support availablecustomizable formsview pricing detailssearch forms by state Have you received the flu vaccine before? I have been given a copy of the vaccine information statement (vis). Influenza (flu) vaccine (inactivated or recombinant): Do any of the following apply? I consent to the administration of the vaccine(s) marked above. Each year a new flu vaccine is made to protect against the influenza viruses believed to be likely to cause disease in the upcoming flu season. Influenza vaccine may be given at the same time as Please be aware you are responsible for knowing your insurance benefits and payment coverage. Administration date administration site left arm right arm nasal left thigh right thigh. (contains thimerosal) complete information about person to receive the vaccine. Influenza vaccine does not cause flu.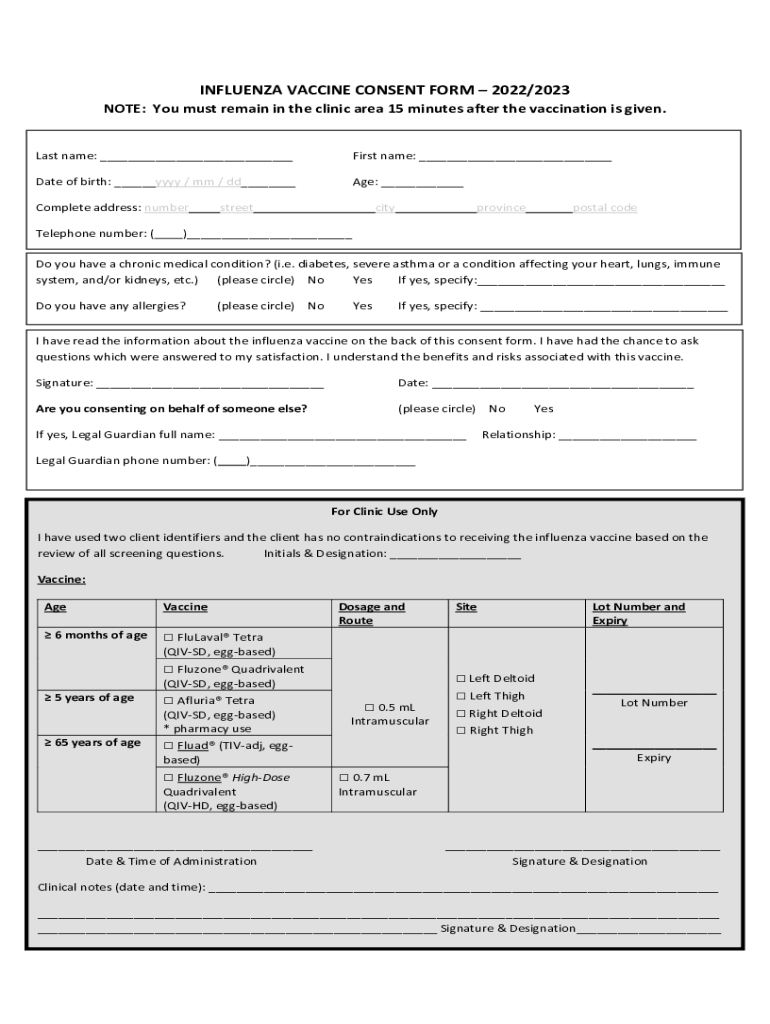
Printable Flu Vaccine Consent 20222024 Form Fill Out and Sign
Flu Vaccine Consent Form Template Jotform

Free printable flu vaccine consent form Fill out & sign online DocHub
Influenza Vaccine Consent FormMust Be Returned to Fill Out and Sign

COVID19 Vaccine Consent Form_spanish_moderna.docx Buena Vista County
Free Printable Flu Vaccine Consent Form

COVID19 Vaccine Informed Consent (General) DIGITAL FORM

Flu Vaccination Consent Form 2 Free Templates in PDF, Word, Excel

Printable Flu Vaccine Consent Form Template
Printable Flu Vaccine Consent Form Printable Word Searches
The Most Common Side Effects Are Tenderness, Swelling And Redness At The Injection Site Which Usually Disappears Within A Few Days.
This Flu Shot Consent Form Is Designed To By Given Out By Medical Professionals And Completed By Patients Agreeing To A Vaccine Against Influenza.
First Second If Second, Please Indicate The Date Of The First Dose:
Understand That Flu Vaccine Is Part Of My Preventive Care Benefit.
Related Post: